Specialised healthcare at Instituto Bernabeu endometriosis unit
Comprehensive, personalised healthcare in order to improve quality of life by reducing pain and preventing potential complications as well as improving and preserving fertility
What is endometriosis and what are its symptoms?
Endometriosis is a disease in which uterine tissue (endometrium) grows outside the uterine cavity. It affects between 10 – 15% of women of childbearing age and can affect up to 50% of women with fertility difficulties. Its cause is still unknown and its influence on fertility may vary. For example, we can see cases with large endometriotic lesions that do not affect fertility and, on the other hand, less significant lesions that cause reproductive disorders.
Sometimes, endometriosis not only causes the uterine tissue -which we call endometrium– to grow outside the uterus, it can also be found in the form of cysts on the ovaries (causing endometriomas), in the fallopian tubes or in any other part of the body except the spleen. These endometriotic implants respond to hormones the same way the endometrium does, so that during menstruation they can grow month after month and even cause slight bleeding and intense pain.
Symptoms
Endometriosis may cause a variety of symptoms. Menstrual cramps are the most common symptoms (dysmenorrhoea), as well as abundant menstrual bleeding and, depending on the implantation location, it can also cause constipation or diarrhoea, haematuria (urinating blood) during menstruation and painful sexual intercourse.
Undoubtedly, one of the symptoms that most worries women with endometriosis is the difficulty in falling pregnant. The reproductive problems it can cause range from repeated miscarriages, embryo implantation problems, ovulation abnormalities and tubal obstruction, amongst others.
Types of endometriosis
The classification most commonly used is the one stablished by the American Society of Reproductive Medicine in 1996:
- Stage I: minimal
- Stage II: mild
- Stage III: moderate
- Stage IV: severe
There are two significant problems with this classification. The first is that there is no link to any fertility problem the patient may have, and the second is that it requires surgery for classification. Therefore, we currently tend to classify endometriosis as follows:
- Superficial: mainly detected after surgery.
- Endometriomas: presence of cysts in ovaries.
- Severe: severe endometrial implants detected after surgery or ultrasound.
Endometriosis treatment at Instituto Bernabeu
One of the problems for patients and doctors is that the pain intensity, its location or duration is not always related to what is seen in the gynaecological ultrasound, so the patient can often feel misunderstood and frustrated as no clear diagnostic findings and no solution to her pain is found.
At Instituto Bernabeu’s Endometriosis Unit, we are pioneers in using the latest advances in diagnosis methods by analysing new reliable biomarkers (immune system indicators): cytokines. In a simple blood sample, we study the mediators involved in the endometriosis inflammatory process, thus generating a precise diagnosis and obtaining highly useful information in terms of the disease’s degree of activity and severity. This means that, in most cases, we are able to avoid diagnostic surgery and the effects this can have on fertility.
Endometriosis correct evaluation and treatment often calls for a multi-disciplinary approach by gynaecologists with experience in diagnostic imaging technology and skilled laparoscopists with experience in Assisted Reproduction.
Years ago, treatment involved mostly surgery. Today, however, we consider we have to be cautious when it affects the ovaries, as the removal of endometriotic tissue entails the loss of valuable ovarian follicles. This leads to a reduction in their functional reserve and, therefore, shortening and reducing the ovarian reserve.
At Instituto Bernabeu, we provide individualised solutions, with several specific research projects in which conventional treatment has been refractory. We also have two specialised units in the major problems caused by endometriosis:
Fertility Preservation: OOCYTES VITRIFICATION
Oocytes vitrification is the technique allowing patients’ own “eggs” to be preserved when they are still young so they can be used when the patient is ready to get pregnant, as the disease can compromise fertility as years go by.
Diagnosis
In the past, the established diagnosis of endometriosis was anatomical-pathological, i.e. the implant had to be removed and, after analysis, confirmed. Nowadays, this aggressive process, which often worsens the couple’s reproductive situation, is no longer necessary.
There has now been a paradigm shift in how endometriosis can be diagnosed. The European Society of Human Reproduction has already established that this diagnosis can be based on the patient’s symptoms alone.
Although questionnaires have not been showed to improve the diagnostic delay of endometriosis, they are considered a useful tool for the patient to consult a doctor if she suspects endometriosis.
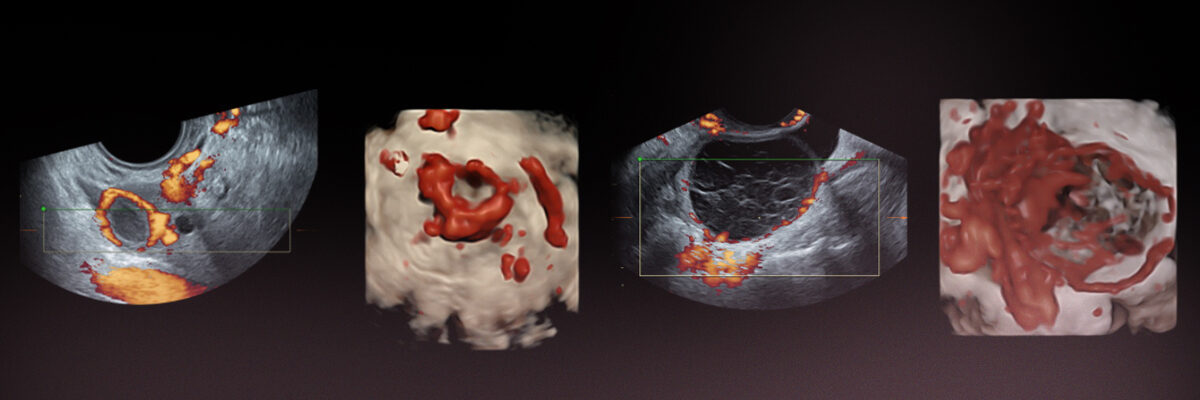
At Instituto Bernabeu we have high-resolution ultrasound scanners that allow us to make an accurate diagnosis. It is true, however, that many of our patients come to us with a perpetuated diagnosis. With our experience, we can better establish the degree of involvement of the disease and its prognosis.
In addition, thanks to our genetics unit we are able to analyse inflammatory mediators called cytokines. Cytokines are proteins produced by various cell types that act as mediators in inflammatory processes and in the immune response. Because of this, they can be considered as biomarkers whose levels can be found to be elevated in case of clinical suspicion of endometriosis.
Likewise, endometriosis has been related to certain variation or polymorphisms in genes which, although it is not yet established which can give a definitive diagnosis, can give us information about the reproductive endometriosis prognosis, such as the VEGF or APOE gene variants, which are currently being analysed in our IBGenRIF test.
Adenomyosis
Adenomyosis is when endometrial tissue is situated within the muscular wall of the uterus (endometriosis in the uterus). This can complicate embryo implantation.
Further to the use of three-dimensional ultrasound equipment in our daily work routine at the clinic, our aim has been to diagnose this little-known pathology.
We are now able to interpret the different images of adenomyosis signs in ultrasounds and one of our lines of investigation is to establish uterine implantation capacity depending on its severity.
What tests are carried out in IB’s Unit for endometriosis treatment?
Endometriosis leads to decreased ovarian reserve as time goes by. We therefore believe it is necessary to first of all carry out a thorough ovarian reserve diagnosis in order to give the patient feedback on the likelihood of falling pregnant in the future. Ovarian reserve is evaluated by means of an antral follicle count, anti-mullerian hormone levels and the patient’s age, amongst other factors.
Depending on the endometriosis severity, pelvic anatomy may be distorted, affecting, amongst other structures, the fallopian tubes. In order to look into this, we perform a hysterosonography (also called sonohysterography) -replacing the hysterosalpingography test- which avoids irradiation of the pelvis and the exploration discomfort.
During the process, and taking into account each patient and all potential benefits, where necessary, a hysteroscopy is a useful procedure in obtaining a direct evaluation of the endometrial cavity and in backing up the information obtained from ultrasound images.

Endocrinology, nutrition and accupuncture for endometriosis
Certain foods can have an effect on the intensity of the disease as well as the increase and decrease of its symptoms. Therefore, the Endometriosis Unit is also given support by our endocrinology and nutrition team in the form of nutritional assessment and advice. The aim is to make the most of natural resources in the fight against the disease and to hold back the associated symptoms.
In order to improve quality of life and by way of a complementary treatment to the endocrinological and gynaecological healthcare being given, acupuncture can help to relieve pain and inflammation which is why we also offer this type of specialised therapeutic support.
Self-diagnosis test. Have i got endometriosis?
Before the age of 10
Between the ages of 11 and 15
Older than 16 years of age
No, never
Yes, sometimes
Yes, always
No, never
Yes, sometimes
Yes, always
No, never
Yes, sometimes
Yes, always
No, never
Yes, sometimes
Yes, always
No, never
Yes, it took me at least 6 months
Yes, I’ve had assisted reproduction treatment
No
I don’t know
Yes
Under 6 tampons/sanitary towels a day
Between 6 and 11 tampons/sanitary towels a day
More than 12 tampons/sanitary towels a day
No
Yes
No
Yes
No
Yes
I have not, but a family member has